|
The
Nobel Assembly at Karolinska Institutet has today
decided to award
The Nobel Prize in
Physiology or Medicine for 2005
jointly to
Barry J. Marshall and J.
Robin Warren
for their discovery
of
"the bacterium
Helicobacter pylori and its role in gastritis and
peptic ulcer disease"
Summary
This year's Nobel
Laureates in Physiology or Medicine made the remarkable and
unexpected discovery that inflammation in the stomach
(gastritis) as well as ulceration of the stomach or duodenum
(peptic ulcer disease) is the result of an infection of the
stomach caused by the bacterium Helicobacter pylori.
Robin Warren (born
1937), a pathologist from Perth, Australia, observed small
curved bacteria colonizing the lower part of the stomach
(antrum) in about 50% of patients from which biopsies had
been taken. He made the crucial observation that signs of
inflammation were always present in the gastric mucosa close
to where the bacteria were seen.
Barry Marshall
(born 1951), a young clinical fellow, became interested in
Warren's findings and together they initiated a study of
biopsies from 100 patients. After several attempts, Marshall
succeeded in cultivating a hitherto unknown bacterial
species (later denoted Helicobacter pylori) from
several of these biopsies. Together they found that the
organism was present in almost all patients with gastric
inflammation, duodenal ulcer or gastric ulcer. Based on
these results, they proposed that Helicobacter pylori
is involved in the aetiology of these diseases.
Even though peptic
ulcers could be healed by inhibiting gastric acid
production, they frequently relapsed, since bacteria and
chronic inflammation of the stomach remained. In treatment
studies, Marshall and Warren as well as others showed that
patients could be cured from their peptic ulcer disease only
when the bacteria were eradicated from the stomach. Thanks
to the pioneering discovery by Marshall and Warren, peptic
ulcer disease is no longer a chronic, frequently disabling
condition, but a disease that can be cured by a short
regimen of antibiotics and acid secretion inhibitors.
Peptic ulcer – an infectious disease!
This year's Nobel
Prize in Physiology or Medicine goes to Barry Marshall and
Robin Warren, who with tenacity and a prepared mind
challenged prevailing dogmas. By using technologies
generally available (fibre endoscopy, silver staining of
histological sections and culture techniques for
microaerophilic bacteria), they made an irrefutable case
that the bacterium Helicobacter pylori is causing
disease. By culturing the bacteria they made them amenable
to scientific study.
In 1982, when this
bacterium was discovered by Marshall and Warren, stress and
lifestyle were considered the major causes of peptic ulcer
disease. It is now firmly established that Helicobacter
pylori causes more than 90% of duodenal ulcers and up to
80% of gastric ulcers. The link between Helicobacter
pylori infection and subsequent gastritis and peptic
ulcer disease has been established through studies of human
volunteers, antibiotic treatment studies and epidemiological
studies.
Helicobacter pylori causes
life-long infection
Helicobacter
pylori is a spiral-shaped Gram-negative bacterium that
colonizes the stomach in about 50% of all humans. In
countries with high socio-economic standards infection is
considerably less common than in developing countries where
virtually everyone may be infected.
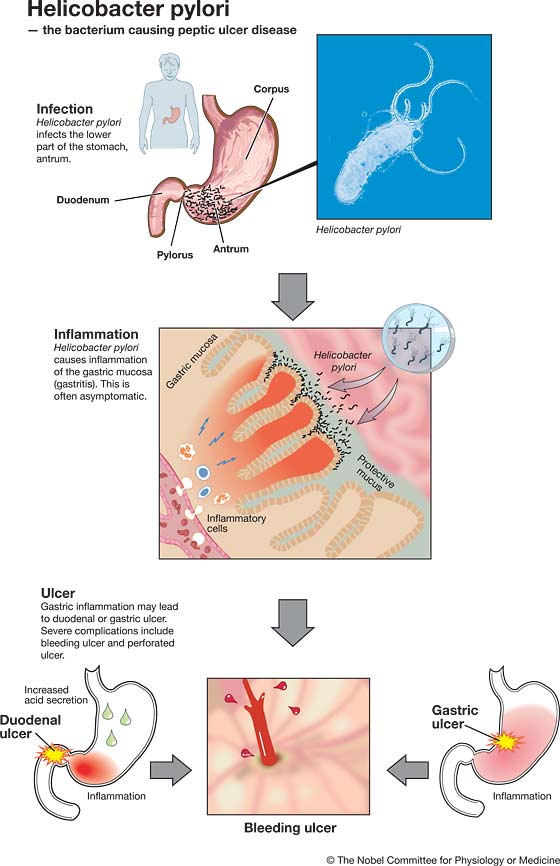
Infection is
typically contracted in early childhood, frequently by
transmission from mother to child, and the bacteria may
remain in the stomach for the rest of the person's life.
This chronic infection is initiated in the lower part of the
stomach (antrum). As first reported by Robin Warren, the
presence of Helicobacter pylori is always associated
with an inflammation of the underlying gastric mucosa as
evidenced by an infiltration of inflammatory cells.
The infection is usually asymptomatic
but can cause peptic ulcer
The severity of
this inflammation and its location in the stomach is of
crucial importance for the diseases that can result from
Helicobacter pylori infection. In most individuals
Helicobacter pylori infection is asymptomatic. However,
about 10-15% of infected individuals will some time
experience peptic ulcer disease. Such ulcers are more common
in the duodenum than in the stomach itself. Severe
complications include bleeding and perforation.
The current view is
that the chronic inflammation in the distal part of the
stomach caused by Helicobacter pylori infection
results in an increased acid production from the
non-infected upper corpus region of the stomach. This will
predispose for ulcer development in the more vulnerable
duodenum.
Malignancies associated with
Helicobacter pylori infection
In some individuals
Helicobacter pylori also infects the corpus region of
the stomach. This results in a more widespread inflammation
that predisposes not only to ulcer in the corpus region, but
also to stomach cancer. This cancer has decreased in
incidence in many countries during the last half-century but
still ranks as number two in the world in terms of cancer
deaths.
Inflammation in the
stomach mucosa is also a risk factor for a special type of
lymphatic neoplasm in the stomach, MALT (mucosa associated
lymphoid tissue) lymphoma. Since such lymphomas may regress
when Helicobacter pylori is eradicated by
antibiotics, the bacterium plays an important role in
perpetuating this tumour.
Disease or not – interaction between
the bacterium and the human host
Helicobacter
pylori is present only in humans and has adapted to the
stomach environment. Only a minority of infected individuals
develop stomach disease. After Marshall's and Warren's
discovery, research has been intense. Details underlying the
exact pathogenetic mechanisms are continuously being
unravelled.
The bacterium
itself is extremely variable, and strains differ markedly in
many aspects, such as adherence to the gastric mucosa and
ability to provoke inflammation. Even in a single infected
individual all bacteria are not identical, and during the
course of chronic infection bacteria adapt to the changing
conditions in the stomach with time.
Likewise, genetic
variations among humans may affect their susceptibility to
Helicobacter pylori. Not until recently has an animal
model been established, the Mongolian gerbil. In this
animal, studies of peptic ulcer disease and malignant
transformation promise to give more detailed information on
disease mechanisms.
Antibiotics cure but can lead to
resistance
Helicobacter
pylori infection can be diagnosed by antibody tests, by
identifying the organism in biopsies taken during endoscopy,
or by the non-invasive breath test that identifies bacterial
production of an enzyme in the stomach.
An indiscriminate
use of antibiotics to eradicate Helicobacter pylori
also from healthy carriers would lead to severe problems
with bacterial resistance against these important drugs.
Therefore, treatment against Helicobacter pylori
should be used restrictively in patients without documented
gastric or duodenal ulcer disease.
Microbial origin of other chronic
inflammatory conditions?
Many diseases in
humans such as Crohn's disease, ulcerative colitis,
rheumatoid arthritis and atherosclerosis are due to chronic
inflammation. The discovery that one of the most common
diseases of mankind, peptic ulcer disease, has a microbial
cause, has stimulated the search for microbes as possible
causes of other chronic inflammatory conditions.
Even though no
definite answers are at hand, recent data clearly suggest
that a dysfunction in the recognition of microbial products
by the human immune system can result in disease
development. The discovery of Helicobacter pylori has
led to an increased understanding of the connection between
chronic infection, inflammation and cancer.
|